A conversation between two sharp minds sparked a realization: how little most people truly understand the complexities of American healthcare. It’s easy to consume headlines and form opinions, but genuine understanding requires lived experience and deep knowledge – a lesson learned from the pitfalls of relying on incomplete information, much like the flawed intelligence used to justify past conflicts.
The issue isn’t a lack of intelligence, but a reliance on narratives crafted by those with agendas. Many academics “covering” healthcare aren’t seeking truth, but constructing stories. And, as any storyteller knows, facts can be inconvenient when a compelling narrative is at stake. This leads to a distorted view of critical issues, like access to healthcare in rural America.
A simple Google search paints a familiar picture: rural healthcare access is “bad.” But beneath the surface lies a decades-long cycle of concern and legislation that hasn’t delivered promised results. Why? Because understanding the current landscape requires unraveling a complex web of laws and, more importantly, how those laws are implemented – a system designed to perpetuate a specific narrative.

The Critical Access Hospital (CAH) designation, born from a wave of rural closures in 1997, provides over 1,300 hospitals with cost-based Medicare reimbursement – essentially, Medicare pays whatever the hospital claims it costs. Subsequent legislation, like the Rural Health Care Access Act, further expanded eligibility, and the Rural Emergency Hospital designation offers additional federal payments. Even Medicare-funded residency slots are allocated specifically for rural hospitals, though a recent report revealed 95% went to institutions that simply reclassified themselves as rural to qualify.
These programs represent significant funding streams, fiercely defended by those who benefit from them. Any attempt to close loopholes or demand accountability is met with resistance, framed as a threat to care for the vulnerable. This creates a powerful incentive to maintain the perception of a rural healthcare crisis, a narrative amplified by academics who consistently rank American healthcare poorly compared to nations with nationalized systems.
But these international comparisons often miss a crucial point: insurance coverage doesn’t equal access. A patient in rural Canada may have universal coverage but face hours-long waits for an ambulance, while a patient in rural Nevada, even uninsured, might reach a cardiac catheterization lab in 40 minutes. Rankings prioritize bureaucratic structures over the reality of timely care, especially in emergencies.
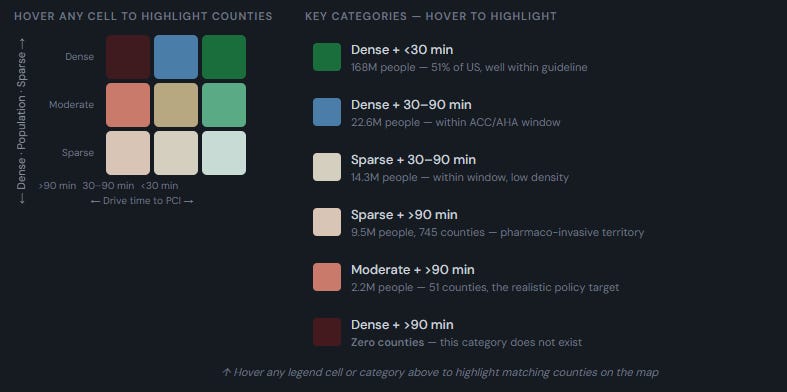
To truly assess the situation, we need concrete metrics. Percutaneous coronary intervention (PCI) – a life-saving procedure for heart attacks – provides an ideal proxy for healthcare access. It’s time-sensitive, requires specialized infrastructure, and has readily available data. If a community can perform PCI within a reasonable distance, it likely has a functioning healthcare ecosystem.
Analyzing data reveals a surprising truth: 84% of Americans live within 60 minutes of a PCI-capable hospital – a level of access unmatched by any other developed nation. However, 11.7 million Americans, primarily in moderate and sparsely populated counties, live beyond the critical 90-minute window. These are the people the legislation aims to help, yet decades of funding haven’t significantly closed the gap.
Comparing the U.S. to Canada, often touted as a model for healthcare reform, reveals a stark contrast. Canada, despite its universal coverage, leaves a far larger percentage of its population – 28.7% – beyond the 90-minute threshold, including over a million people in densely populated areas. The American system, despite its flaws, demonstrably provides better geographic access to emergency cardiac care.

The problem isn’t simply a lack of funding, but a flawed system that rewards institutions for maintaining the perception of a crisis. The solution isn’t to emulate Canada’s system, but to address the underlying issues within our own. This includes incentivizing local physicians to practice in rural communities, tying funding to measurable access outcomes, and breaking the hospital industry’s monopoly on healthcare delivery.
Allowing physicians to own and operate facilities, as demonstrated by successful models like Atlas Surgery Center, could revolutionize rural healthcare. Removing the physician hospital ownership ban would empower local doctors to build and staff hospitals tailored to their communities’ needs, fostering competition and driving down costs.
The path forward requires cutting through the noise of biased narratives and focusing on data-driven solutions. The crisis narrative is a product, manufactured by those who profit from it. A clear understanding of the true scope of the problem is the first step towards building a healthcare system that truly serves all Americans.