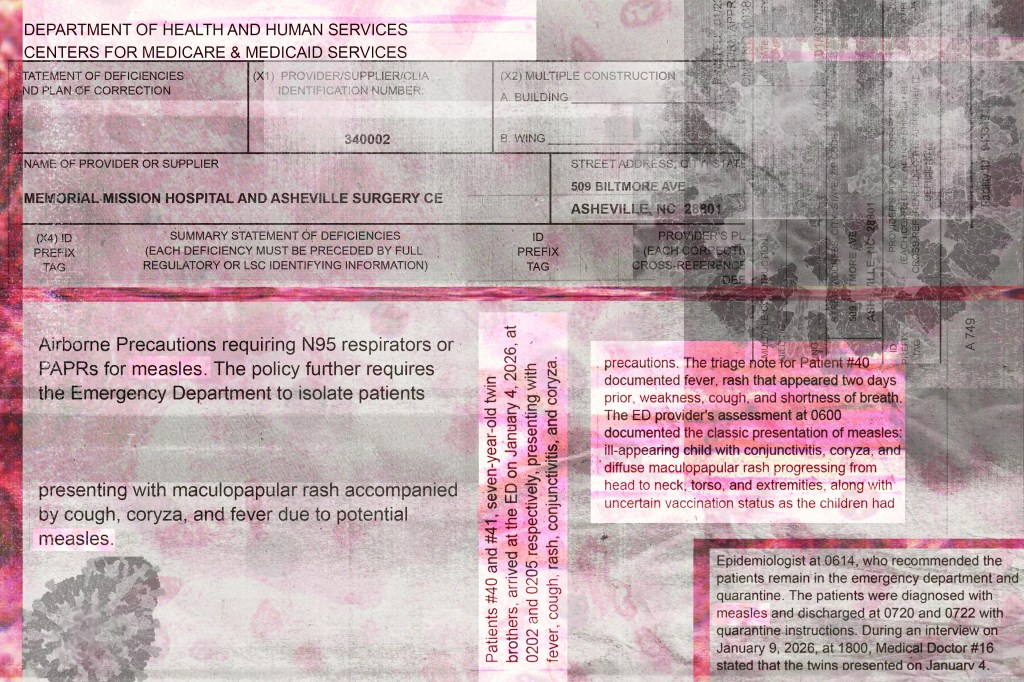
The call came in the early hours. Two seven-year-old twin boys arrived at Mission Hospital in Asheville, North Carolina, exhibiting a constellation of alarming symptoms: fever, cough, a spreading rash, pink eye, and the familiar signs of a common cold. What began as a routine emergency room visit would soon expose a dangerous vulnerability in the nation’s defenses against a once-eradicated foe.
For over two hours, the boys waited – first in one waiting room, then another. Twenty minutes stretched into forty, then eighty, before they were finally isolated. Another two hours ticked by, precious time lost as a potentially highly contagious illness circulated within the hospital walls. As the sun began to rise, an emergency room doctor, increasingly concerned, contacted the state epidemiologist.
The doctor’s description of the symptoms triggered an immediate directive: quarantine the children. Shortly after, the diagnosis arrived – measles. A virus most doctors hadn’t encountered in decades had returned, and its presence would trigger a cascade of consequences, revealing a troubling lack of preparedness.
The hospital sent the family home with instructions for quarantine, unaware of the extent of the exposure. Federal investigators later determined that at least 26 other people within the hospital had been potentially infected that day. Health inspectors discovered a critical failure: the twins’ symptoms should have triggered a hospital-wide isolation protocol, a procedure staff had been trained on just seven months prior.
The Centers for Medicare & Medicaid Services (CMS) swiftly designated Mission Hospital in “Immediate Jeopardy,” one of the most severe sanctions possible, threatening to withhold federal funding. The hospital maintained its staff was trained to handle airborne illnesses and adhered to federal guidelines, but the damage was done.
Across the country, hospitals are facing a growing risk of measles outbreaks, and a surprising obstacle is emerging: many healthcare workers simply don’t recognize the disease. A “morbilliform” rash – a measles-like rash – can be caused by numerous viruses, making accurate diagnosis incredibly difficult, even for experienced pediatricians who have never seen a confirmed case.
North Carolina has already reported over 20 cases since mid-December, part of a nationwide surge exceeding 3,000 infections since the beginning of 2025. Outbreaks are concentrated in areas with low immunization rates, prompting urgent public health campaigns to promote vaccination. The stakes are clear: with two doses of the MMR vaccine, the risk of infection after exposure drops to just 3%, compared to a staggering 90% for the unvaccinated.
However, a troubling trend has undermined public trust in vaccines. Over the past year, policies have cast doubt on their effectiveness. The appointment of a longtime anti-vaccine activist to a key health position, and subsequent changes to recommended vaccination schedules, have fueled skepticism and contributed to declining immunization rates.
Following a measles outbreak in West Texas, the same official publicly advocated for unproven treatments – steroids, antibiotics, and cod liver oil – alarming infectious disease experts and leaving healthcare workers to rely on their own judgment and guidance from state public health systems. The ability to quickly and accurately identify measles, a disease that can initially mimic a common cold, is now paramount.
Officially, the U.S. has maintained “measles elimination status” since 2000, but that status is now in jeopardy. Outbreaks in multiple states are pushing the nation toward losing this designation, a consequence of sustained viral spread exceeding established limits. One county in South Carolina, just an hour from Asheville, has already reported over 900 cases – more than the entire state of Texas saw in 2025.
Measles is a highly contagious virus that attacks the lungs and airways, causing fever, cough, a blotchy rash, and red, watery eyes. It can remain active in the air for up to two hours after an infected person leaves a room, and carries a mortality rate of 1 to 3 deaths per 1,000 cases in children. Tragically, two children in Texas and one adult in New Mexico have already succumbed to the virus in 2025.
The CDC provides detailed diagnostic guidance and state agencies are developing tracking dashboards, but a simple rule of thumb has emerged: look for the three C’s – cough, coryza (cold symptoms), and conjunctivitis (pink eye). Mission Hospital staff had even received training on these key indicators, yet failed to act swiftly enough in the case of the twins. The CDC recommends immediate isolation in a specially equipped room, a precaution that was not followed, with patients separated only by plastic partitions.
Despite the challenges, many healthcare professionals are adapting. Patsy Stinchfield, a former president of the National Foundation for Infectious Diseases, acknowledges the difficulty of identifying measles amidst a sea of winter respiratory illnesses. She described the CMS penalty for Mission Hospital as “extreme,” given the inherent diagnostic complexities.
However, a growing concern is a perceived lack of support from the CDC. Health workers report a disconnect, a decline in communication and guidance that began shortly after a change in leadership. One pediatrician in Asheville has implemented a screening process in the parking lot, while another expressed frustration with parents dismissing measles as a harmless childhood illness.
In North Carolina’s Buncombe County, health officials have already counted seven cases and anticipate a surge. They fear a trajectory similar to South Carolina, where a gradual accumulation of cases could quickly escalate into a widespread outbreak. Local officials are actively urging vaccination, debunking misinformation, and updating parents on the evolving situation.
The situation demands a renewed commitment to public health, a coordinated response, and a clear message about the importance of vaccination. As one pediatrician poignantly stated, “We can’t change the past. All we can do is try to educate and move forward.”